Ebola Disease: Current Situation
- CDC
- 7th August 2025
New developments
- To date, no Ebola cases associated with this outbreak have been reported in the United States, and the risk to the general public remains low.
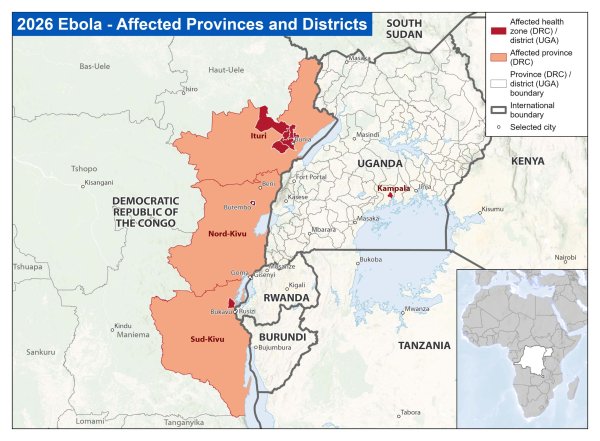
- As of May 23, the DRC and Uganda Ministries of Health report the following:
- A new confirmed case in Sud-Kivu Province; previously, cases had been confirmed in Ituri and Nord-Kivu provinces only.
- DRC: A total of 746 suspected cases, 83 confirmed cases, 176 suspected deaths, and 9 confirmed deaths.
- Uganda: A total of 5 confirmed cases and 1 confirmed death.
- On May 23, Uganda announced 3 additional cases, all with clear links to the previously announced cases in people who traveled from DRC.
- This is a rapidly evolving situation, and case counts are subject to change.
- On May 17, an American who was exposed as part of work caring for patients in DRC tested positive for Ebola Bundibugyo disease. The patient has been transported to Germany for treatment and care. In addition to being a shorter flight time, Germany has previous experience caring for Ebola patients.
- High-risk contacts associated with this exposure have been moved to Germany and the Czech Republic.
- On May 18, CDC, the Department of Homeland Security, and other appropriate federal agencies took proactive public health measures to prevent Ebola from entering the United States.
- More information about enhanced travel security measures is available:
Background
- In early May, a hospital in Bunia Health Zone in northeastern DRC identified a cluster of severe illnesses affecting healthcare workers.
- Initial samples tested in DRC were negative for Ebola virus, but by May 15, 8 out of 13 samples tested positive, and 5 were inconclusive. Using genetic fingerprinting, the illnesses were identified as Bundibugyo (Bun-dee-BOO-joh) virus, one of the 4 types of orthoebolaviruses that cause Ebola disease in people.
- There is no vaccine for Bundibugyo virus, and treatment consists of supportive care.
- There have been 2 previous outbreaks of Bundibugyo virus, 1 in Uganda (2007) and 1 in DRC (2012), with death rates of 25% and 50%, respectively.
- Patients have experienced classic Ebola disease symptoms like fever, headache, vomiting, severe weakness, abdominal pain, nosebleeds, and vomiting blood.
- In DRC, most cases to date have been in people between 20 and 39 years old, and two-thirds have been in female patients.
- This is the 17th outbreak of Ebola in DRC since 1976. The most recent outbreak ended in December 2025.
CDC response
CDC is working with international partners and the Ministries of Health on this evolving situation. CDC is further supporting response efforts through our country offices in DRC and Uganda to provide technical assistance with:
- Disease tracking and contact tracing
- Laboratory sample collection and virus sequencing
- Infection prevention and control (IPC) efforts
- Local border screening
- Coordinating with affected countries and international public health partners
- Providing personal protective equipment (PPE) and infection control supplies
- Risk communication and community engagement in affected areas
CDC is working with other U.S. Government agencies and international partners to move the American who tested positive for Ebola on May 17 and other Americans at high risk out of DRC for care.
In the United States
- CDC has travel health notices in place for DRC and Uganda to help Americans planning travel to either country in the near future learn how to keep themselves safe from Ebola.
- CDC is taking proactive public health measures to prevent Ebola from entering the United States, including:
- Enhancing public health screening and traveler monitoring for individuals arriving from the DRC, Uganda, and South Sudan
- Putting entry restrictions on non-U.S. passport holders if they have been in Uganda, DRC, or South Sudan in the previous 21 days
- Coordinating with airlines, international partners, and port-of-entry officials to identify and manage travelers who may have been exposed to Ebola
- Enhancing port health protection response activities, contact tracing, laboratory testing capacity, and hospital readiness nationwide
- Continuing deployment of CDC personnel to support outbreak containment efforts in affected regions
- CDC has extensive clinical guidance and training for both U.S. and non-U.S. settings, including Infection Prevention and Control Recommendations for Patients in U.S. Hospitals who are Suspected or Confirmed to have Selected Viral Hemorrhagic Fevers.
- CDC is also coordinating with health departments nationwide to:
- Follow established patient assessment protocols if BVD is suspected in a patient with concerning clinical and epidemiologic history.
- Coordinate patient management, specimen collection, and BVD testing with state, tribal, local, and territorial health departments, CDC, and clinical teams.
- CDC is also supporting U.S. Government interagency efforts to coordinate the safe withdrawal of a small number of Americans who are directly affected in outbreak areas.
- Long-standing laboratory preparedness efforts are online for suspected viral hemorrhagic fevers like Ebola to allow for testing directly at CDC or through one of 41 Laboratory Response Network public health laboratories.


No comments yet!